
To augment existing literature with more diverse methodologies, we took a more holistic approach than prior reviews of stunting reduction in Nepal, triangulating across literature reviews, quantitative analyses, and qualitative inquiry.
Literature review
We initiated our research process with a systematic literature review of contextual factors, national and subnational interventions, policies, strategies, programs, and other initiatives that may have contributed to reductions in child stunting over time. Broad searches, followed by de-duplication and predefined exclusions, resulted in a total of 114 records with information pertinent to child stunting in Nepal.
Quantitative analysis
Quantitative methods involved (1) descriptive analyses to provide contextual understanding of the stunting decline across geographic, socioeconomic, gender, and age segments and (2) linear multivariable regression-based difference-in-difference analysis and regression-based decomposition analyses to understand the major predictors of the stunting decline, as well as their relative importance to Nepal’s progress. We utilized multiple data sources: Nepal’s Demographic and Health Surveys (DHS), other national household surveys (MICS), census data, and data from specific programs, at the household, ecological (subnational-level), and national levels.
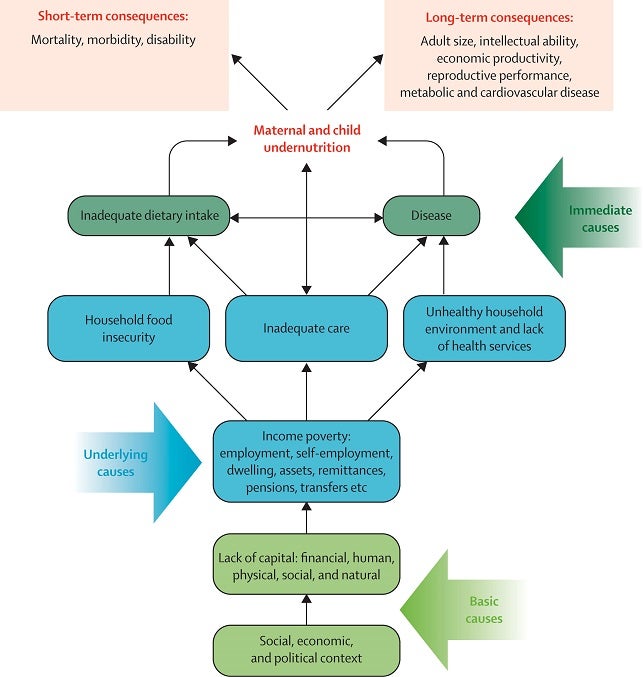
We organized available variables for analysis into a conceptual framework adapted from the UNICEF / Lancet nutrition series undernutrition conceptual framework, which groups determinants of stunting into their causal hierarchical levels.
UNICEF / Lancet nutrition series conceptual framework
Descriptive analysis
To explore geospatial within-region stunting variation, we utilized five-by-five kilometer area stunting estimates modeled by the Institute of Health Metrics and Evaluation (IHME). IHME used Nepal DHS and MICS datasets incorporated into Bayesian spatial models to generate posterior predicted prevalence of stunting. The model draws strength from covariables, years, and locations where data is available.
To examine inequalities across population subgroups, we examined stunting, as well as coverage of relevant interventions, across important subnational dimensions: wealth quintile, level of maternal education, area of residence (urban or rural), child gender, and wealth quintile by area of residence.
Finally, to examine the growth faltering process from birth to five years of age, we estimated child growth curves also known as Victora curves. Smoothed polynomial curves were used to plot predicted child height-for-age Z-scores against child age to assess growth trajectories and gain an understanding of how stunting risk changes with age.
Linear multivariable regression (difference-in-difference analysis)
The linear multivariable regression is based on a difference-in-difference analysis framework to evaluate if a change in a proposed predictor of HAZ leads to a change in HAZ over the studied time period. Using DHS data, we analyzed the four surveys - 2001, 2006, 2011, and 2016 - for children under five years of age.
To examine the association between HAZ and various indicators, we conducted a series of step-wise linear regression models. A hierarchical modelling approach using distal, intermediate and proximal level variables was executed as suggested by Victora 1997 to generate the final multivariable models. Variables within each level were selected from our general conceptual framework.
Step 1 was a series of bivariate regressions to determine crude associations between indicators in our conceptual framework and HAZ outcome. Step 2 was to use all candidate variables for multivariable model building (i.e., with p-value ≤0.20) irrespective of their direction to move forward for multivariable modeling. Bivariate correlations estimate the absolute crude associations between the covariable and the outcome, and they highlight the total (unadjusted) effect of the factor on HAZ. In multivariable analysis, the final multivariable regression coefficient is adjusted for child age, sex and region (control variables) and all confounders in preceding levels.
Oaxaca-Blinder decomposition
Our Oaxaca-Blinder decomposition analysis is based largely on individual and household-level data, with larger sample sizes and higher statistical power. We focused on index mother-child pairs (i.e., the youngest child and youngest mother in any given household). This standard approach simplifies modeling and interpretation with minimal loss in data. Again, we analyzed the 2001-2016 time period and applied a similar hierarchical modeling approach as used for the difference-in-difference analysis.
We used height-for-age Z-score (HAZ) as the outcome of interest. The analysis was stratified by child age group (<6 months, 6-23 months, all children under five).
Importantly, the Oaxaca-Blinder decomposition allowed us to identify the relative contribution of each predictive factor to HAZ change. We did this by using a linear least square regression model, accounting for survey design and weights, to assess associations between HAZ, time, control variables (i.e., child age and sex), and any trend effects.
Qualitative analysis
Focus group discussion and in-depth interviews
To investigate a diverse range of stakeholder perspectives (e.g. national experts, mothers, health care workers, etc.), we conducted a series of in-depth interviews with national stakeholders and held a set of focus group discussions with community health workers and mothers.
A total of 18 key national-level informants were interviewed. Profiles ranged from nutrition experts, representatives from donor organizations, ministries and state agencies, among others. Respondents were asked to describe key nutrition-specific and -sensitive events in Nepal as well as comment on key trends and contextual factors that impacted child undernutrition over time. Ten community representatives, including Female Community Health Volunteers (FCHVs), were also interviewed to provide community-level perspectives and experiences on transitions in nutrition and stunting.
Focus group discussions were also conducted in the Thecho and Dukucchap communities Lalitpur District, in Province 3. Women that had given birth in 1995-2000 and 2010-2015 were recruited to participate.
Policy and program review
To understand implementation of policies, programs, and strategies, we conducted additional research and corroborated our findings with country experts. A similar multi-pronged data collection and corroboration exercise was undertaken to track financial data linked to the nutrition policy and program timeline.