
To augment existing literature, we took a more holistic approach than prior reviews of stunting reduction in Peru, triangulating across literature reviews, quantitative analyses, and qualitative inquiry.
Literature review
We initiated our research process with a systematic literature review of contextual factors, national and subnational interventions, policies, strategies, programs, and other initiatives that may have contributed to reductions in child stunting over time. Broad searches, followed by de-duplication and predefined exclusions, resulted in a total of 134 records with information pertinent to child stunting in Peru.
Quantitative analysis
Quantitative methods involved (1) descriptive analyses to provide contextual understanding of the stunting decline across geographic, socioeconomic, gender, and age segments and (2) hierarchical multivariable regression and regression-based decomposition analyses to understand the major predictors of the stunting decline, as well as their relative importance to Peru’s progress. We utilized multiple data sources: Peru’s Demographic and Health Surveys (DHS), other national household surveys (ENAHO), census data, and data from specific programs, at the household, ecological (subnational-level), and national levels.
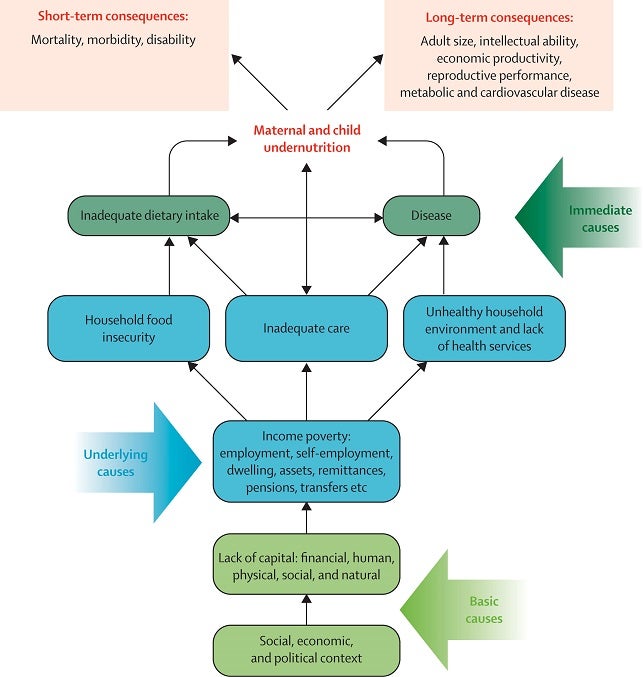
We organized available variables for analysis into a conceptual framework adapted from the UNICEF / Lancet nutrition series undernutrition conceptual framework, which groups determinants of stunting into their causal hierarchical levels.
UNICEF / Lancet nutrition series undernutrition conceptual framework
Lancet series: Interventions in undernutrition
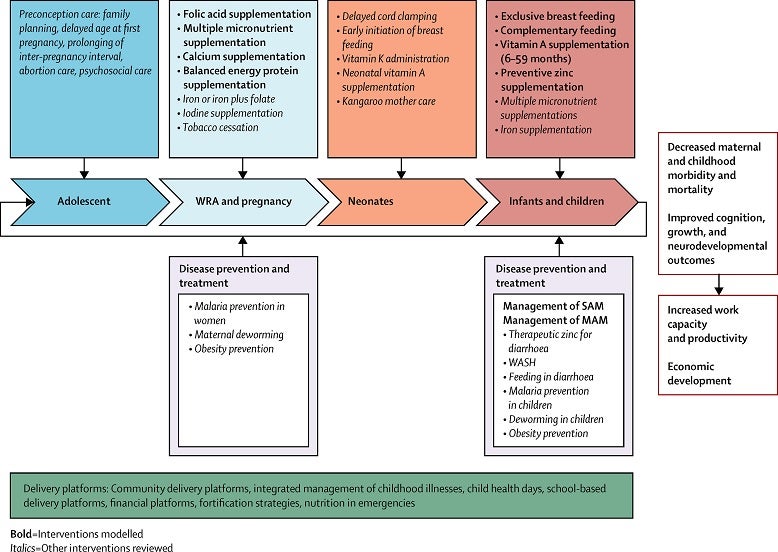
Bhutta ZA, Das JK, Rizvi A, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? The Lancet. 2013;382(9890):452-477. doi:10.1016/s0140-6736(13)60996-4.
Conceptual framework showing distal, intermediate, and proximal determinants of stunting

Descriptive analysis
To explore geospatial within-region stunting variation, we utilized five-by-five kilometer area stunting estimates modeled by the Institute of Health Metrics and Evaluation (IHME). IHME used Peru DHS datasets incorporated into Bayesian spatial models to generate posterior predicted prevalence of stunting. The model draws strength from covariables, years, and locations where data is available.
To examine inequalities across population subgroups, we worked with the International Center for Equity in Health, in Pelotas, Brazil, to estimate stunting in Peru across important subnational dimensions: wealth quintile, level of maternal education, area of residence (urban or rural), child gender, and geographic region (administrative and broader states).
Finally, to examine the growth faltering process from birth to five years of age, we estimated child growth curves also known as Victora curves. Smoothed polynomial curves were used to plot predicted child height-for-age z-scores against child age to assess growth trajectories and gain an understanding of how stunting risk changes with age.
Linear mixed effects regression
The linear mixed effects regression is a time-series ecological analysis using region-year data (i.e., each data point is a region-level estimate for one given year) and two-year lagged stunting prevalence as the outcome. Using DHS data, we analyzed three time periods: 2000-2016, 2000-2007, and 2008-2016, with 2007 serving as a natural inflection point due to Peru’s sharp decline in stunting prevalence starting in that year.
We used a hierarchical modeling approach in line with our adapted conceptual framework to account for the mediation of distal factors by proximal causes. The model accounted for the fixed effects of predictors and time; the random effects account for variability within and between states, as well as over time. Finally, we included a two-year time lag between predictive variables and outcome variable (stunting prevalence), given the time necessary for interventions and other factors to make an impact.
We modeled at the region-level to counteract individual characteristics (especially poverty) which are not well measured in surveys and can result in confounding (i.e., any determinant associated with poverty is identified as a predictor of stunting). However, this methodology makes inferences susceptible to ecological fallacy (i.e., correlations between variables at the group level do not always translate into correlations at the individual level).
Oaxaca-Blinder decomposition
Our Oaxaca-Blinder decomposition analysis is based largely on individual and household-level data, with larger sample sizes and higher statistical power. We focused on index mother-child pairs (i.e., the youngest child and youngest mother in any given household). This standard approach simplifies modeling and interpretation with minimal loss in data. Again, we analyzed three time periods: 2000-2016, 2000-2007, and 2008-2016 and applied a similar hierarchical modeling approach as used for the linear mixed effects model.
We selected height-for-age z-score (HAZ) rather than child stunting (i.e., yes or no) as the outcome of interest for greater statistical efficiency. The analysis was stratified by child age group (<6 months, 6-23 months, 24-59 months, all children under five).
Importantly, the Oaxaca-Blinder decomposition allowed us to identify the relative contribution of each predictive factor to HAZ change. We did this by using a linear least square regression model, accounting for survey design and weights, to assess associations between HAZ, time, control variables (i.e., child age and sex), and any trend effects.
Qualitative analysis
Focus group discussion and in-depth interviews
To understand national stakeholder perspectives, we conducted a focus group discussion followed by a series of in-depth interviews.
We initiated our qualitative inquiry with a ~100-minute-long focus group discussion conducted by two members of the research team at the Universidad Peruana Cayetano Heredia (UPCH). Six participants were selected among recognized representatives of institutions considered key in the effort to reduce child stunting in Peru. The focus group discussion helped to identify specific points that required additional exploration during the follow-up ten individual interviews.
Key informants for individual interviews were selected based on their experience in areas or institutions that were instrumental in the design and implementation of interventions to reduce child stunting in Peru. We generally did not repeat participants in each of the activities.
Policy and program review
To understand implementation of policies, programs, and strategies, we conducted additional research and corroborated our findings with country experts. A similar multi-pronged data collection and corroboration exercise was undertaken to track financial data linked to the nutrition policy and program timeline.
For a more detailed explanation of our methodology, please review the narrative PDF