
KEY POINTS
The success of the Programa Articulado Nutricional (PAN) was due to both the design of the program as well as its implementation. Diving into the details of implementation reveal the following:
CRED
Child growth monitoring visits (CRED visits, as they were called) involved counseling of mothers on child nutrition best practices, including exclusive breastfeeding, hand washing, and complementary feeding. Children were expected to have completed 23 CRED visits by the time they turned three years old.
PAN budget
The largest single share of the PAN budget was allocated toward introducing and rapidly scaling coverage of pneumococcal conjugate vaccine (PCV) and rotavirus vaccine.
PAN expenditures
PAN has been a well-funded program almost since its inception. Since 2009, PAN expenditures have ranged from $425 million to over $650 million annually.
Early days
Program targeting was especially important in the early days of the program. From 2008 to 2010, the program prioritized the 16 states with the highest stunting rates and incidence of poverty. In particular, the initial budget directed funds to the poor, high-burden states of Apurímac, Ayacucho, Cajamarca, Huánuco and Huancavelica.
DHS Program
An expanded DHS program and other information systems were used to track funding allocation, expenditure, and impact. This data informed annual government reports on progress, as well as monitoring and evaluation by civil society organizations. They also contributed to twice yearly strategic and tactical discussions, as well as rewards and incentives for strong performance.
The Programa Articulado Nutricional (PAN) is a results-based financing program that coordinates efforts across multiple Peruvian government ministries. Its goal is to reduce childhood stunting by decreasing incidence of low birth weight, improving nutrition of children under three, and reducing infection. The tools and background material in this section are provided to help users understand the implementation of PAN.
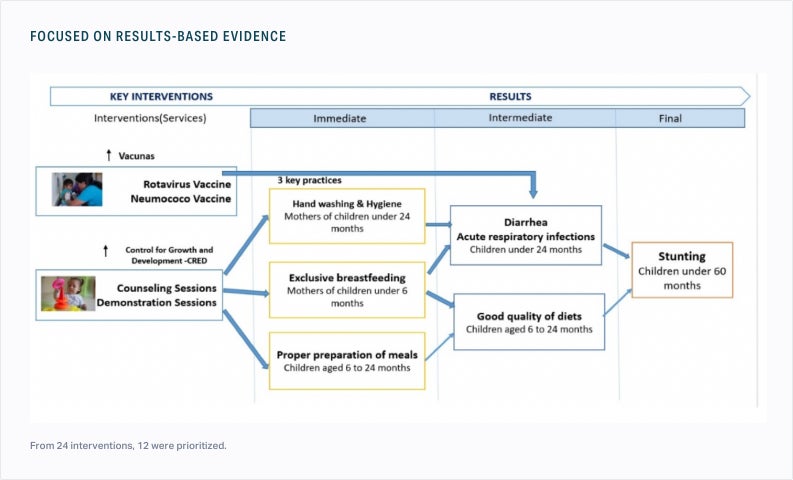
Logic model: Programa Articulado Nutricional (PAN)

Peru Ministry of Economics and Finance (MEF)
Full program design
Of the 24 total interventions, the Peruvian government prioritized three from the start: child growth monitoring (“ control de crecimiento y desarollo,” or “CRED” for short), nutrition and hygiene counseling for mothers, and the introduction of pneumococcal conjugate vaccine (PCV) and rotavirus vaccine. One additional intervention - iron supplementation for children and pregnant women - was intended for prioritization, but ran into challenges in implementation.
PAN expenditure by priority, 2009-2016, USD, millions

Provided by Luis Cordero, formerly of the Peruvian Ministry of Health (MINSA)
The above visualization illuminates how the interventions prioritized by PAN (CRED - which included counseling for mothers - and immunization) received increases in funding. Immunization and CRED consistently account for the largest portions of expenditure. Other important priorities include support of complementary feeding (delivered primarily through growth monitoring sessions) and care for acute respiratory infections and diarrheal disease. Iron supplementation, for both children and pregnant women, occupies a small but gradually increasing portion of expenditure.
Child growth monitoring (CRED)
Growth monitoring sessions are considered the most important strategy for improving child health and nutrition. A typical session lasts 45 minutes and starts with the child being measured and weighed. During the same visit, mothers receive counseling. The subject of counseling varies with the age of the child and includes exclusive breastfeeding, hand washing, and complementary feeding for children between six and twelve months. In addition, CRED programming also provides mothers with cooking classes focused on preparing nutritious meals with locally available ingredients and classes on how to care for their children during times of illness.




Tactically, health workers are taught best practices for CRED by a team of nurses and social workers that travel the country organizing training programs. Health workers are taught to use short, clear statements to communicate; they spread the message that malnutrition should be prevented in addition to being treated and that breastfeeding should continue even after solid food is introduced when a baby turns six months old.
These lessons are reinforced continually. A total of thirteen CRED sessions are recommended in the first year of a child’s life (at seven and fifteen days, followed by one per month from one to eleven months of age); between twelve and 23 months, toddlers are monitored every other month; between ages two and three, children have four more check-ups. As such, a child with complete CRED at 36 months would have had more than twenty visits to a health facility; his or her mother would have had the same number (or more) of counseling sessions with a health worker. Despite the large number of visits required for “complete” CRED, the percentage of Peruvian children under 36 months with completed growth monitoring regimens has reached nearly 60 percent.
Pneumococcal and rotavirus vaccination
PAN funding allowed for an increase in the supply of vaccines that were already a part of Peru’s immunization schedule (e.g., BCG, DPT, polio, measles). Most of the additional PAN funding for vaccines, however, was allocated to supporting the introduction of two new vaccines to the immunization schedule: PCV and rotavirus. These vaccines were prioritized based on disease burden and international experience, which showed that reducing acute respiratory infection and diarrheal disease - the illnesses that most significantly inhibit child nutrient absorption - would have the biggest impact on reducing chronic malnutrition. Both vaccines were introduced in 2009, initially in the poorest states in the country.

Funding and geographic focus
Budget over time
PAN allocated budget and expenditure, 2009-2016, USD

Peru Ministry of Economics and Finance (MEF), 2017. PAN allocated budget and expenditure (USD) [dataset]. Government of Peru; 2017. Accessed 2017
Expenditure on PAN has ranged from $425 million to over $650 million annually.
Geographic focus
From 2008 to 2010, the 16 states with the highest stunting rates and incidence of poverty were prioritized for PAN implementation. In particular, the initial budget directed funds to the poor, high-burden states of Apurímac, Ayacucho, Cajamarca, Huánuco and Huancavelica. As the program matured, PAN continued to allocate more spending to areas with greater stunting burden, but its reach was nationwide.
Monitoring and evaluation
Data and accountability
Prior to 2007, Peru conducted USAID-funded Demographic and Health Surveys (DHS) every three to five years, like many other low-and middle-income countries. Since 2007, Peru has conducted DHS annually with samples broad and large enough to be statistically significant at the state level. Subnational data allows the government and civil society organizations to pinpoint overachieving states for recognition and underperforming states for strategic or tactical changes.
Beyond DHS, Peru utilizes multiple information systems to gather, evaluate and assess information related to malnutrition:
- The Sistema Integrado de Administracion Financiera (SIAF) is used for budget allocations
- The Sistema Integrado de Gestión Administrativa (SIGA) is used for inputs at the health facility level
- The Sistema de Padron Nominado monitors individual children with services provided
These data are used to track funding allocation, expenditure, and impact. PAN provides government and civil society stakeholders with an annual report on its progress on reducing stunting; the IDI and MCLCP also monitor and evaluate the program independently. Civil society leaders and local governments meet every six months to discuss progress and challenges.

EUROPAN
From 2009 through 2014, the European Commission agreed to contribute up to $72 million (62 million Euro) to a program called EUROPAN, which provided funding incentives to regional governments to expedite PAN’s roll out and impact.
The EU’s budget support was conditional: disbursements to Peru were only made if the country demonstrated compliance with commitments around general economic and fiscal policy, as well as other PAN-specific goals. The $72 million was an upper cap; Peru would not receive that total amount in funding until it demonstrated success. Funding from EUROPAN came in two categories:
- Fixed tranche funding: awarded for fulfillment of best-practice logistical and administrative processes (e.g., hiring of staff); these were assessed every six months
- Variable tranches: awarded based on achievement of intervention coverage goals; these were assessed annually
Visual explanation of European tranche funding & requirements

In addition to prioritizing coverage of PCV, rotavirus vaccine, and child growth monitoring, the Peruvian government under EUROPAN committed to improving coverage of iron supplementation among both children and pregnant women. For each of these interventions, EU prioritized equity: it awarded variable tranche funding for improving coverage for the lowest wealth quintile.
Initially, EUROPAN prioritized three of the poorest, highest-burden states: Apurímac, Ayacucho and Huancavelica. Eventually, EUROPAN expanded its scope to encompass six states. The states that met their EUROPAN goals received enough support to increase their nutrition budgets by up to 50 percent.